Vocal Cord Complications After Intubation
May 25, 2026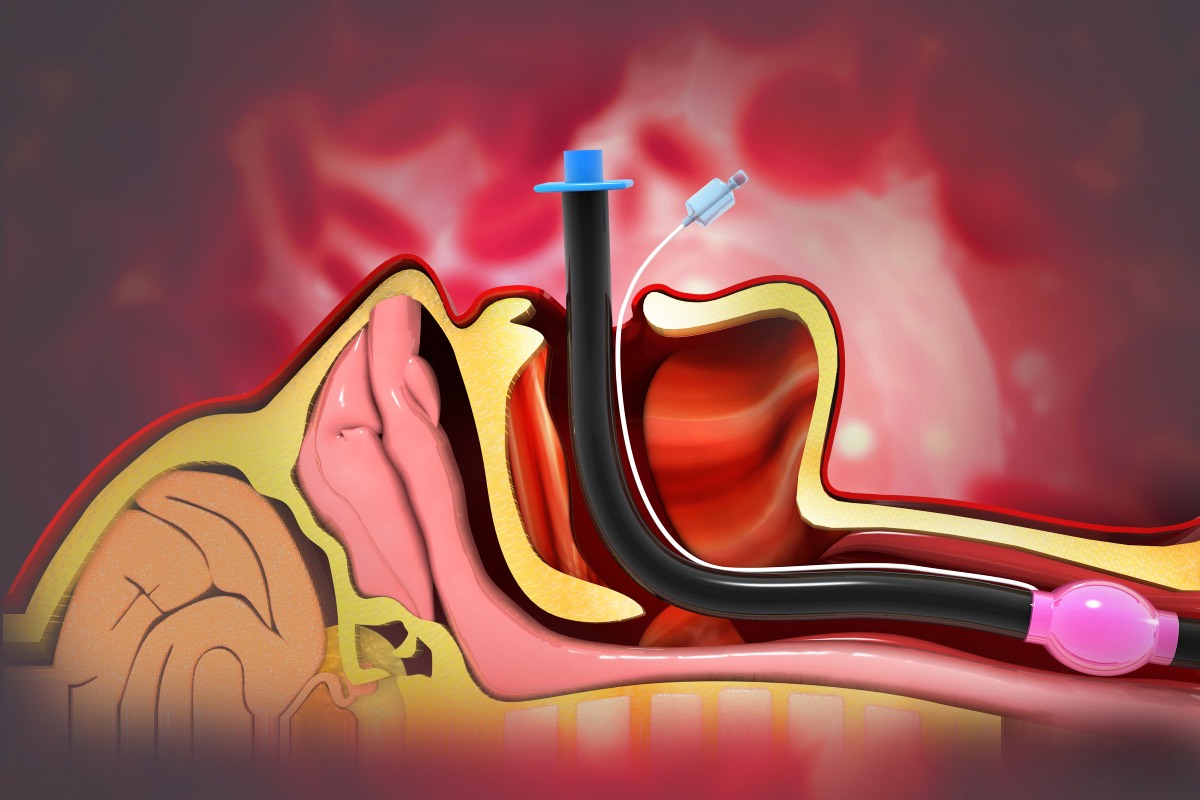
Endotracheal intubation is a life-saving procedure that facilitates control of airflow, can help manage pulmonary complications of disease, and help to stabilize people in the immediate aftermath of severe trauma to the airway or to the breathing centers of the brain. However, as with any invasive procedure, it is not without risk to the patient. Because endotracheal tubes must pass through the vocal cords during intubation, complications relating to them may occur. They can range from relatively benign, common side effects like transient hoarseness, to more serious ones like vocal fold immobility. These complications are influenced by patient comorbidities, tube management, and duration of intubation.
Hoarseness is one of the most common complications of endotracheal intubation related to the vocal cords, affecting as many as 71% of patients after general anesthesia according to one study (Hurtado Nazal et al., 2018). Hoarseness is usually self-limited, lasting only about 3–4 days. However, in about 1% of patients, the hoarseness can be permanent, usually due to laryngeal damage sustained during the intubation procedure. In more severe cases where the patient sustains vocal cord paralysis, it is typically attributed to recurrent laryngeal nerve compression, more commonly on the left. The recurrent laryngeal nerves provide innervation to all but one of the intrinsic muscles of the larynx and are therefore critical to the production of normal speech.
There are several identified risk factors in predicting the likelihood of vocal cord paralysis. These include relatively common comorbidities like type II diabetes mellitus, hypertension, and peripheral vascular disease, as well as perioperative complications, such as experiencing hypotension and requiring vasopressor administration while intubated (Campbell et al., 2020).
Interestingly, both of the aforementioned studies note a left-sided predominance in cases of vocal cord paralysis. This can potentially be attributed to the more commonly employed right-sided fixation of endotracheal tubes, which results in the angling of the tube to the left and the long-term compression of the left recurrent laryngeal nerve rather than the right. Vocal cord paralysis can limit more than speech production. It can also impair the cough reflex, resulting in increased risk for aspiration both peri- and postoperatively.
Complications of endotracheal intubation extend beyond mechanical compression. Other commonly encountered complications are granulomatous inflammation of airway cartilage caused by mucosal trauma from tube insertion, as well as posterior glottic stenosis, caused by fibrotic changes resulting from long-term endotracheal tube intubation resulting in an extended inflammatory process and fibrosis (Woo et al., 2023).
When hoarseness persists beyond the typical 72-hour postoperative window, clinical intervention becomes necessary to differentiate between simple edema and nerve damage. The gold standard for diagnosis is laryngeal videostroboscopy, which allows clinicians to visualize vocal fold symmetry and mucosal wave patterns. If unilateral impairment is confirmed, management often begins conservatively with speech therapy to strengthen compensatory mechanisms. For structural issues like intubation granulomas, a combination of inhaled steroids and proton pump inhibitors (PPIs) is frequently prescribed to reduce the inflammatory “scrubbing” effect of gastric reflux on the injured tissue (Woo et al., 2023). In refractory cases or instances of severe posterior glottic stenosis, surgical intervention—such as laser excision or airway reconstruction—may be required to restore patency.
Preventing iatrogenic laryngeal injury requires a multifaceted approach to tube management. Anesthesiologists and ICU staff must prioritize frequent monitoring of cuff pressure to ensure a seal without compromising mucosal capillary blood flow. Furthermore, using appropriately sized tubes and minimizing the duration of intubation can significantly reduce the risk of permanent fibrosis. While endotracheal intubation remains an indispensable tool in critical care, awareness of its potential for vocal cord or laryngeal trauma and complications is essential. By identifying high-risk patients with vascular comorbidities and responding promptly to persistent dysphonia, clinicians can mitigate the long-term functional impact on a patient’s voice and airway safety.
References
- Campbell, B. R., et al. (2020). Unilateral Vocal Fold Immobility After Prolonged Endotracheal Intubation. JAMA Otolaryngology–Head & Neck Surgery, 146(2), 160. https://doi.org/10.1001/jamaoto.2019.3969
- Hurtado Nazal, C., et al. (2018). Vocal cord paralysis after endotracheal intubation: an uncommon complication of general anesthesia. Brazilian Journal of Anesthesiology, 68(6), 637-640. https://doi.org/10.1016/j.bjane.2017.12.007
- Woo, J. H. (2023). Treatment Results of Vocal Process Granuloma: Intubation versus Contact Granuloma. Journal of Clinical Medicine (via PMC10147457).