Malignant Hyperthermia Precautions for High-Risk Patients
June 29, 2026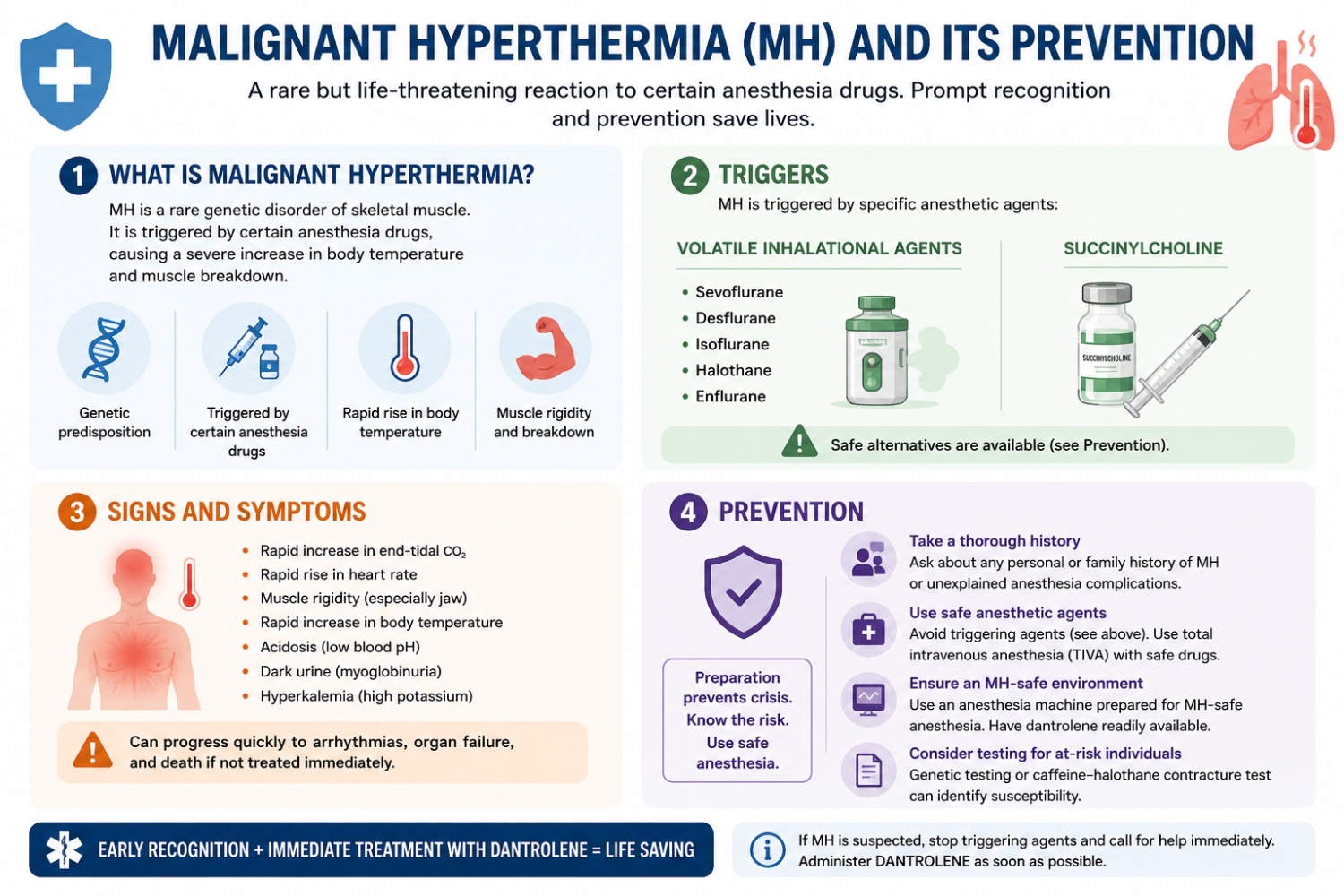
Malignant hyperthermia (MH) is a life-threatening musculoskeletal crisis that can occur in susceptible individuals undergoing anesthesia. Patients at high risk for malignant hyperthermia, particularly those with a family history of the disorder or underlying genetic conditions such as central core disease, may experience catastrophic hypermetabolic reactions if exposed to triggering anesthetic agents. Therefore, it is critical to have precautions in place for such patients. Eliminating malignant hyperthermia-related mortality requires thorough preoperative screening, strict trigger-free anesthetic protocols, vigilant monitoring, and immediate crisis readiness for at-risk individuals.
Malignant hyperthermia is characterized by a severe hypermetabolic reaction of skeletal muscle to certain anesthetic agents. The disorder is most commonly associated with mutations in the RYR1 gene, which encodes a receptor involved in calcium regulation during muscle contraction. In susceptible individuals, exposure to triggering agents causes excessive calcium release within skeletal muscle cells, resulting in sustained muscle contraction, increased oxygen consumption, excessive carbon dioxide production, and rapid heat generation. If untreated, MH can lead to serious complications, including cardiac arrhythmias, rhabdomyolysis, acute kidney injury, and death.
Several critical screening measures can help reduce the risk of MH. Obtaining a detailed family history of adverse reactions to anesthesia is an essential first step because MH is often inherited. Although the documented incidence of malignant hyperthermia is relatively low, estimated at 0.18–3.9 cases per 100,000 general anesthetics, the prevalence of genetic susceptibility is much higher, with approximately 1 in 1,000 individuals carrying a predisposing mutation (Tsutsumi et al., 2025). Preoperative screening should include questions regarding family members who experienced unexplained fevers, muscle rigidity, or complications during surgery. In addition, assessing for a family history of congenital myopathies is important because certain conditions are strongly associated with malignant hyperthermia susceptibility. Patients with uncharacterized neuromuscular disorders should undergo further evaluation before surgery (Tsutsumi et al., 2025).
Several precautions must be implemented in the operating room to ensure patient safety. As a precaution, triggering agents, including succinylcholine and volatile anesthetics such as sevoflurane and halothane, should be fully avoided in patients at risk for malignant hyperthermia. Anesthesia machines must be properly prepared before surgery by removing vaporizers and flushing the system with high-flow oxygen or by using activated charcoal filters to reduce residual anesthetic gases (Billmen & Gillies, 2014). Safe alternatives include total intravenous anesthesia with propofol, local or regional anesthesia, and non-depolarizing neuromuscular blocking agents (Malignant Hyperthermia Association of the United States [MHAUS], n.d.).
Perioperatively, the anesthesiologist is responsible for closely monitoring the patient for signs of malignant hyperthermia. Although muscle rigidity is a classic manifestation, it is not present in all cases. Early warning signs may include unexplained tachycardia, hypercarbia, hyperkalemia with peaked T waves on electrocardiography, cola-colored urine due to myoglobinuria, and rapidly increasing body temperature. Prompt recognition of these symptoms is essential because early intervention significantly improves outcomes (Larach et al., 2014).
In addition to preventive measures, immediate access to dantrolene is essential. Dantrolene is the only specific treatment for malignant hyperthermia and acts by inhibiting calcium release from the sarcoplasmic reticulum, thereby reducing excessive muscle contraction and metabolic activity. The availability of dantrolene has dramatically reduced mortality, decreasing death rates from greater than 70% before its introduction to less than 5% in modern practice. Facilities that administer triggering anesthetic agents must maintain an adequate supply of dantrolene and ensure that personnel are trained in its rapid preparation and administration (MHAUS, n.d.).
Malignant hyperthermia remains a rare but potentially fatal anesthetic complication. Thorough preoperative screening, trigger-free techniques, equipment preparation, vigilant monitoring, and immediate availability of dantrolene significantly reduce the risk of severe complications and mortality and are critical precautions when providing anesthesia to patients with a high risk of malignant hyperthermia.
References
- Tsutsumi YM, Nagasaka H, Mukaida K, et al. JSA guideline for management of malignant hyperthermia in 2025. J Anesth. 2026;40(1):4-12. doi:10.1007/s00540-025-03647-y.
- Bilmen JG, Gillies RL. Clarifying the role of activated charcoal filters in preparing an anaesthetic workstation for malignant hyperthermia-susceptible patients. Anaesth Intensive Care. 2014;42(1):51-58.
- Malignant Hyperthermia Association of the United States. (n.d.). Recommendations for the management of malignant hyperthermia. https://www.mhaus.org
- Larach MG, Brandom BW, Allen GC, Gronert GA, Lehman EB. Malignant hyperthermia deaths related to inadequate temperature monitoring, 2007–2012: A report from the North American Malignant Hyperthermia Registry. Anesth Analg. 2014;119(6):1359-1366.